I shared this pic on the Facebook page a little while ago and it had a lot of interaction.
I've done some research on this lately and thought I'd share what I found here with you.
I'm not sharing this information as a tool for you to self-diagnose...you're not qualified ;)...but I am sharing it for your educational and informational benefit.
If any of the following sounds familiar to what you are feeling and living with...
please speak to a qualified professional.
I've done some research on this lately and thought I'd share what I found here with you.
I'm not sharing this information as a tool for you to self-diagnose...you're not qualified ;)...but I am sharing it for your educational and informational benefit.
If any of the following sounds familiar to what you are feeling and living with...
please speak to a qualified professional.
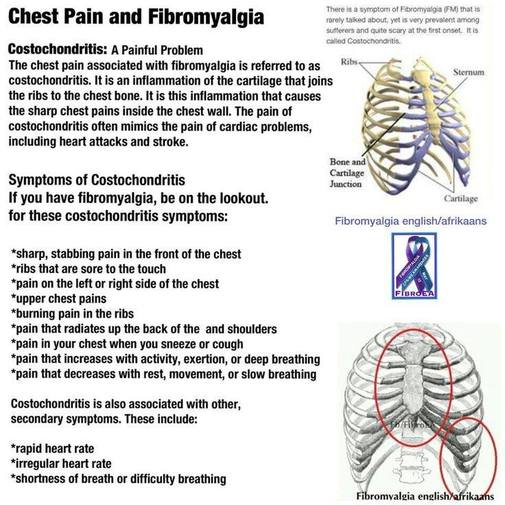
Costochondritis Overview
Costochondritis is an inflammation of the junctions where the upper ribs join with the cartilage that holds them to the breastbone, or sternum. The condition causes localized chest pain that you can reproduce by pushing on the cartilage in the front of your ribcage. Costochondritis is a relatively harmless condition and usually goes away without treatment. The cause is usually unknown, but may happen from increased activity involving the arms.
·Costochondritis (with unknown cause) is a common cause of chest pain in children and adolescents. It accounts for 10% to 30% of all chest pain in children. Annually, doctors evaluate about 650,000 cases of chest pain in young people ages 10 to 21. The peak age for the condition is ages 12-14.
·Costochondritis is also considered as a possible diagnosis for adults who have chest pain. Chest pain in adults is considered a potentially serious sign of a heart problem by most doctors until proven otherwise. Chest pain in adults usually leads to a battery of tests to rule out heart attack and heart disease. If those tests are normal and your physical exam is consistent with costochondritis, your doctor will diagnose costochondritis as the cause of your chest pain. It is important, however, for adults with chest pain to be examined and tested for heart disease before being diagnosed with costochondritis. It is often difficult to distinguish between the two without further testing. The condition affects females more than males (70% versus 30%). Costochondritis may also occur as the result of an infection or as a complication of surgery on your sternum.
·Tietze syndrome is often referred to as costochondritis, but the two are distinct conditions. You can tell the difference by noting the following:
·Tietze syndrome usually comes on abruptly, with chest pain radiating to your arms or shoulder and lasting several weeks. Tietze syndrome is accompanied by a localized swelling at the painful area (the junction of the ribs and breastbone).
Costochondritis Causes
Costochondritis is an inflammatory process but usually has no definite cause. Repeated minor trauma to the chest wall, overuse of the arms, or viral respiratory infections can commonly cause chest pain due to costochondritis. Occasionally, costochondritis as a result of bacterial infections can occur in people who use IV drugs or who have had surgery to their upper chest. After surgery, the cartilage can become more prone to infection, because of reduced blood flow in the region that has been operated on.
Different types of infectious diseases can cause costochondritis.
Costochondritis Symptoms
Chest pain associated with costochondritis is usually preceded by exercise, minor trauma, or an upper respiratory infection.
·The pain usually will be sharp and located on your front chest wall. It may radiate to your back or abdomen and is more common on your left side.
·The most common sites of pain are your fourth, fifth, and sixth ribs. This pain increases as you move your trunk or take deep breaths. Conversely, it decreases as your movement stops or with quiet breathing.
·The reproducible tenderness you feel when you press on the rib joints (costochondral junctions) is a constant feature of costochondritis. Without this tenderness, a diagnosis of costochondritis is unlikely.
·Tietze syndrome, on the other hand, exhibits swellings at the rib-cartilage junction. Costochondritis has no noticeable swelling. Neither condition involves pus or abscess formation.
·Tietze syndrome usually affects the junctions at the second and third ribs. The swelling may last for several months. The syndrome can develop as a complication of surgery on your sternum months to years after the operation.
·When costochondritis occurs as a result of infection after surgery, you will see redness, swelling, or pus discharge at the site of the surgery.
When to Seek Medical Care
Call the doctor for any of the following symptoms:
Go to a hospital's emergency room if you have difficulty breathing or any of the following symptoms occur. These symptoms are generally not associated with costochondritis:
Exams and Tests for Costochondritis
Costochondritis does not lend itself to diagnosis by tests. Personal history and a physical exam are the mainstays of diagnosis. However, tests are sometimes used to rule out other conditions that can have similar symptoms but are more dangerous, such as heart disease.
·The doctor will seek to reproduce tenderness over the affected rib joints, usually over the fourth to sixth ribs in costochondritis, and over the second to third ribs in Tietze syndrome. In costochondritis with unknown causes, there is no significant swelling of costochondral joints.
·There is swelling and tenderness of the rib-cartilage junctions in Tietze syndrome. Although some doctors use the terms costochondritis and Tietze syndrome interchangeably, Tietze syndrome has a sudden onset without any preceding respiratory illness or any history of minor trauma. In Tietze syndrome, there is frequently radiation of pain to arms and shoulders, as well as pain and tenderness associated with swelling at the spot that hurts.
·Blood work and a chest X-ray are usually not helpful in diagnosing costochondritis. However, after sternum surgery, or for people at risk for heart disease, doctors will be more likely to do tests if you have chest pain and possible costochondritis to be certain you do not have any infection or other serious medical problems. To determine if infection is the cause of chest pain, doctors will:
·Look for signs of infection such as redness, swelling, pus, and drainage at the site of surgery
·Order a more sophisticated imaging study of the chest called a gallium scan, which will show increased uptake of the radioactive material gallium in an area of infection
·Check the white blood cell count to see if it is elevated, a sign of infection
·Order a chest X-ray if pneumonia is a suspected cause of chest pain
·Order an ECG and other tests if a heart problem is suspected
·Costochondritis is a less common cause of chest pain in adults but occurs fairly frequently in people who have had cardiac surgery. The diagnosis can only be reached after excluding more serious causes of chest pain that are related to the heart and lungs. The appropriate studies, such as ECG, chest X-rays, blood test for heart damage, and other studies will be done as indicated. Any chest pain in adults is taken seriously and not ignored. If you are concerned, consult with your doctor.
Home Remedies for Costochondritis
Medications for Costochondritis
Surgery for Costochondritis
Surgical removal of the sore cartilage may be required if there is no response to medical therapy for costochondritis. Your doctor will refer you to a surgeon for consultation should this option be considered necessary.
Next Steps
Costochondritis Treatment Follow-up You should see a doctor during recovery, and then once a year. Infectious costochondritis requires long-term observation.
Costochondritis Prevention
Because inflammatory costochondritis has no definite cause, there is no good way to prevent it.
Costochondritis Outlook
Noninfectious costochondritis will go away on its own, with or without anti-inflammatory treatment. Most people will recover fully.
Infectious costochondritis responds well to IV antibiotics and surgical repair, but recovery may take a long time.
WebMD Medical Reference from eMedicineHealth
Reviewed by David Kiefer, MD on January 03, 2014
© 2014 WebMD, LLC. All rights reserved.
Costochondritis is an inflammation of the junctions where the upper ribs join with the cartilage that holds them to the breastbone, or sternum. The condition causes localized chest pain that you can reproduce by pushing on the cartilage in the front of your ribcage. Costochondritis is a relatively harmless condition and usually goes away without treatment. The cause is usually unknown, but may happen from increased activity involving the arms.
·Costochondritis (with unknown cause) is a common cause of chest pain in children and adolescents. It accounts for 10% to 30% of all chest pain in children. Annually, doctors evaluate about 650,000 cases of chest pain in young people ages 10 to 21. The peak age for the condition is ages 12-14.
·Costochondritis is also considered as a possible diagnosis for adults who have chest pain. Chest pain in adults is considered a potentially serious sign of a heart problem by most doctors until proven otherwise. Chest pain in adults usually leads to a battery of tests to rule out heart attack and heart disease. If those tests are normal and your physical exam is consistent with costochondritis, your doctor will diagnose costochondritis as the cause of your chest pain. It is important, however, for adults with chest pain to be examined and tested for heart disease before being diagnosed with costochondritis. It is often difficult to distinguish between the two without further testing. The condition affects females more than males (70% versus 30%). Costochondritis may also occur as the result of an infection or as a complication of surgery on your sternum.
·Tietze syndrome is often referred to as costochondritis, but the two are distinct conditions. You can tell the difference by noting the following:
·Tietze syndrome usually comes on abruptly, with chest pain radiating to your arms or shoulder and lasting several weeks. Tietze syndrome is accompanied by a localized swelling at the painful area (the junction of the ribs and breastbone).
Costochondritis Causes
Costochondritis is an inflammatory process but usually has no definite cause. Repeated minor trauma to the chest wall, overuse of the arms, or viral respiratory infections can commonly cause chest pain due to costochondritis. Occasionally, costochondritis as a result of bacterial infections can occur in people who use IV drugs or who have had surgery to their upper chest. After surgery, the cartilage can become more prone to infection, because of reduced blood flow in the region that has been operated on.
Different types of infectious diseases can cause costochondritis.
- Viral: Costochondritis commonly occurs with viral respiratory infections because of the inflammation of the area from the viral infection itself, or from straining from coughing.
- Bacterial: Costochondritis may occur after surgery and be caused by bacterial infections.
- Fungal: Fungal infections are rare causes of costochondritis.
Costochondritis Symptoms
Chest pain associated with costochondritis is usually preceded by exercise, minor trauma, or an upper respiratory infection.
·The pain usually will be sharp and located on your front chest wall. It may radiate to your back or abdomen and is more common on your left side.
·The most common sites of pain are your fourth, fifth, and sixth ribs. This pain increases as you move your trunk or take deep breaths. Conversely, it decreases as your movement stops or with quiet breathing.
·The reproducible tenderness you feel when you press on the rib joints (costochondral junctions) is a constant feature of costochondritis. Without this tenderness, a diagnosis of costochondritis is unlikely.
·Tietze syndrome, on the other hand, exhibits swellings at the rib-cartilage junction. Costochondritis has no noticeable swelling. Neither condition involves pus or abscess formation.
·Tietze syndrome usually affects the junctions at the second and third ribs. The swelling may last for several months. The syndrome can develop as a complication of surgery on your sternum months to years after the operation.
·When costochondritis occurs as a result of infection after surgery, you will see redness, swelling, or pus discharge at the site of the surgery.
When to Seek Medical Care
Call the doctor for any of the following symptoms:
- Trouble breathing
- High fever
- Signs of infection such as redness, pus, and increased swelling at the rib joints
- Continuing or worsening pain despite medication
- Nausea
- Sweating
Go to a hospital's emergency room if you have difficulty breathing or any of the following symptoms occur. These symptoms are generally not associated with costochondritis:
- High fever not responding to fever-reducers such as acetaminophen(Tylenol) or ibuprofen (Advil)
- Signs of infection at the tender spot, such as pus, redness, increased pain, and swelling
- Persistent chest pain of any type associated with nausea, sweating, left arm pain, or any generalized chest pain that is not well localized. These may be signs of a heart attack. If you are not sure what is causing your condition, always go to the emergency room.
Exams and Tests for Costochondritis
Costochondritis does not lend itself to diagnosis by tests. Personal history and a physical exam are the mainstays of diagnosis. However, tests are sometimes used to rule out other conditions that can have similar symptoms but are more dangerous, such as heart disease.
·The doctor will seek to reproduce tenderness over the affected rib joints, usually over the fourth to sixth ribs in costochondritis, and over the second to third ribs in Tietze syndrome. In costochondritis with unknown causes, there is no significant swelling of costochondral joints.
·There is swelling and tenderness of the rib-cartilage junctions in Tietze syndrome. Although some doctors use the terms costochondritis and Tietze syndrome interchangeably, Tietze syndrome has a sudden onset without any preceding respiratory illness or any history of minor trauma. In Tietze syndrome, there is frequently radiation of pain to arms and shoulders, as well as pain and tenderness associated with swelling at the spot that hurts.
·Blood work and a chest X-ray are usually not helpful in diagnosing costochondritis. However, after sternum surgery, or for people at risk for heart disease, doctors will be more likely to do tests if you have chest pain and possible costochondritis to be certain you do not have any infection or other serious medical problems. To determine if infection is the cause of chest pain, doctors will:
·Look for signs of infection such as redness, swelling, pus, and drainage at the site of surgery
·Order a more sophisticated imaging study of the chest called a gallium scan, which will show increased uptake of the radioactive material gallium in an area of infection
·Check the white blood cell count to see if it is elevated, a sign of infection
·Order a chest X-ray if pneumonia is a suspected cause of chest pain
·Order an ECG and other tests if a heart problem is suspected
·Costochondritis is a less common cause of chest pain in adults but occurs fairly frequently in people who have had cardiac surgery. The diagnosis can only be reached after excluding more serious causes of chest pain that are related to the heart and lungs. The appropriate studies, such as ECG, chest X-rays, blood test for heart damage, and other studies will be done as indicated. Any chest pain in adults is taken seriously and not ignored. If you are concerned, consult with your doctor.
Home Remedies for Costochondritis
- Pain relievers such as nonsteroidal anti-inflammatory medications like ibuprofen (Advil, Motrin) or naproxen (Aleve) as needed
- Local heat or ice to relieve pain
- Avoiding unnecessary exercise or activities that make the symptoms worse; avoid contact sports until there is improvement in symptoms, and then return to normal activities only as tolerated.
Medications for Costochondritis
- Costochondritis responds to nonsteroidal anti-inflammatory medications such as ibuprofen (Advil or Motrin) and naproxen (Aleve).
- You may be given a local anesthetic and steroid injection in the area that is tender if normal activities become very painful and the pain does not respond to drugs.
- Infectious (bacterial or fungal) costochondritis should be treated initially with intravenous (in the vein or IV) antibiotics. Afterward, antibiotics by mouth or by IV should be continued for another two to three weeks to complete the therapy.
Surgery for Costochondritis
Surgical removal of the sore cartilage may be required if there is no response to medical therapy for costochondritis. Your doctor will refer you to a surgeon for consultation should this option be considered necessary.
Next Steps
Costochondritis Treatment Follow-up You should see a doctor during recovery, and then once a year. Infectious costochondritis requires long-term observation.
Costochondritis Prevention
Because inflammatory costochondritis has no definite cause, there is no good way to prevent it.
Costochondritis Outlook
Noninfectious costochondritis will go away on its own, with or without anti-inflammatory treatment. Most people will recover fully.
Infectious costochondritis responds well to IV antibiotics and surgical repair, but recovery may take a long time.
WebMD Medical Reference from eMedicineHealth
Reviewed by David Kiefer, MD on January 03, 2014
© 2014 WebMD, LLC. All rights reserved.
 RSS Feed
RSS Feed
